Narrative And Experience Transformed
for the University of Texas Medical School's Series on Narrative in Art and Medicine,
UT-Houston Medical School, 6431 Fannin at Ross Sterling Blvd., Rm 2.006, Thursday, April 3, 1997
by John H. Lienhard
Mechanical Engineering Department
University of Houston
Houston, TX 77204-4792
jhl [at] uh.edu (jhl[at]uh[dot]edu)
Last time we talked about narrative and healing. Today, let's pick up a related idea: To understand the place of narrative in medicine, it may help to understand the metaphors that shape medicine in the first place.
To see how metaphor shapes technology, I'll start, not with medicine, but with clocks: The circular face of a sundial, its shadow moving left to right, was copied into water-clock faces — hands moving around a twelve-hour dial.
Then, around AD 1300, the tick-tock mechanical escapement radically improved clock accuracy and compactness. But, changed as they were, clocks still had dials, bells, and gears. Medieval writers said almost nothing about the new mechanism inside, so historians still aren't exactly sure when that change took place.
You see, the outward form, the clock face, could not change, because that's where the metaphor was expressed.
Around 1920 we replaced mechanical escapements with the steady oscillation of alternating current. Accuracy took another leap forward, but clocks still looked the same.
My quartz crystal watch not only has the circular face of a sundial or a water clock; it also has a second hand that moves in little jumps as though it were controlled by an escapement mechanism. Designers know, on a visceral level, that the meeting ground between user and machine should change as little as possible.
So what about digital clocks? They offer a more precise readout than analog clocks. They're easier for children to read. Linear time — time as a sequence of rising numbers — that's pure simplicity, but it's simplicity in the same way a tree is simpler than a forest.
Circular dials paint a picture of Earth's rotation. They model our experience of passing time. They're a lovely analog of reality. In a digital display, night never falls. Time just advances, without features, minute after minute.
The competition between analog and digital readout might seem to balance. But, what do you wear on your wrists? The fascinating truth is, the digital clock has already lost in that competition. Digital clocks simply can't compete with the metaphorical power and visual grace of the circling motion of an analog face.
Many technologies look good for a while, then get left — Betamax, dirigibles, LP's, autogyros, and digital clocks. So what does survive, and why? To predict the death or survival of a technology you certainly must ask if it's functional. But that, by itself, is never enough.
You have to ask if it's a metaphor for something more than function. Only after a technology has touched us as metaphor will it find a way to persist from one generation to the next.
Try another technology — the book. The book, as we know it, was developed by the Attilids in Pergamon when the Egyptians cut off their papyrus supply. They had to begin writing on sheepskin. And it lends itself better to being folded into pages and sewn into a book than being rolled into a scroll the way papyrus was.
The book turned out to be a splendid new compact information-storage medium — so good, it created a new technological metaphor. But bear in mind that the scroll, which it replaced, survives, even today, as its own technological metaphor. But the book was a whole new user interface, and one we will not give up today.
When Gutenberg began printing with movable type, he made print look just like the work of scribes. He counterfeited manuscript books. We still replicate the old manuscript books today. We fold pages into gatherings, sew gatherings together, and lace them between hard covers. Movable type made books cheap and abundant. Yet we readers still receive information just the way we did in Pergamon, 2000 years ago.
Friends ask me, "How much change will we undergo?" Well, where the user meets the machine is the one place we won't tolerate change, even though the machine itself is mutating into something so different as to redirect human history.
Once the machine becomes metaphor, the user interface stops changing. When I work at my computer, I use the awkward old QWERTY typewriter keyboard. A century-old arrangement. The place where I meet the machine, imperfect as it is, remains, and it will not be abandoned.
Pianos evolved from harpsichord improvements. But they were soon something wholly different. Pianos are so different from harpsichords that you still need a harpsichord when you want to hear harpsichord music.
All the best technologies survive their replacements that way. Live concerts survive recordings. Pens survive word processors.
In 1990, everyone expected to be reading electronic books in the near future. Now computers have already leap-frogged that technology. Before we had a decent electronic book, the world-wide-web was on its way to providing everything we might ever hope to get from one:
Screen resolution and illustrations are improving, the supply of texts is rocketing upward. Now we have both sound and motion.
As we leave the limitations of the paper book, its electronic equivalent is already unrecognizably different. And that's exactly why the paper book will have to survive after all. Paper books will keep right on doing what they've always done so well. They take you into the author's mind. You give yourself over to her story-telling rhythm.
Your mind frames the pictures and plays the music. You feel organic cloth and paper against your fingers. What the computer offers has as much in common with the paper book as the horseless carriage has in common with the horse.
But what do paper books have that computers won't soon have as well? Fix the screen, fix the portability, find means for dog-earing your place, then what's left? The answer lies in the metaphor. Not only has the book long since found its metaphorical place in our lives, the computer has found its metaphorical place as well.
The book is our metaphorical mentor.
The computer is our metaphorical servant.
We all switch between the roles of parent and child. We need some control over things, but we also need to submit to other people's knowledge. In some things, we should play the parent. In others, we'd better know how to be a child. And the child says, "Tell me a story."
The story we choose might be a Gothic novel. It might be a math textbook. In either case we give ourselves over to the story-teller for a time. We do that when we read a book, go to the theater, even listen to a concert.
Computer communications are quite another matter. The computer does our bidding. We say, "Go and do. Buy me an airplane ticket. Give me a stock quotation. Tell me if the library has a book. Pass this message to a friend." The computer dances to our tune. We are in control.
When you and I go to the computer for text material, it's to look things up. It's not to let words wash over us. The computer is far better than a book if you want to find things.
Insofar as paper books function as simple repositories of fact — dictionaries, handbooks, indexes, — they've already given way to computers. But the sort of book we submit ourselves to will have to remain written out and uncontrollable.
To learn, we become as children. We seek out our own ignorance. Now and then we follow the mind of someone who knows what we do not. We yield to the rhythm of the story-teller.
Printed books let us put control aside for a while. That's the wonderful gift books offer. But the metaphor of the computer has already been set. Whatever we can do with electronic media, we simply will not use them as mentors.
Now, what has all this to do with medicine and narrative? Last time, one of you asked me about Scott Montgomery's book, The Scientific Voice. That question drives right to the heart of the matter. Let's look at his argument:
Montgomery dives into the language of science, and what he finds is anything but scientific detachment. He tracks the way the language of science bends science itself to fit cultural norms and metaphors.
He gives examples: psychology, Japanese science, how we've studied the moon in terms of the language we use to describe it. Then there's his chapter on medicine and language.
Example, when Harvey studied blood flow in the 17th century, most people thought blood made one pass through the body — that it was generated, then consumed, in various tissues. Harvey showed that blood moved in a closed loop, and he called that motion circulation. But he wasn't first. When others suggested a closed loop, it hadn't caught on. Blood didn't circulate until Harvey gave us the right word.
A huge shift took place in the metaphors of modern medicine around 1870, and Louis Pasteur had a lot to do with it. Early-19th-century doctors still said the plague infected people or lay upon them. It didn't attack them or strike them down. That's what armies did, not diseases.
When Pasteur was young, disease was caused by an excess of irritation or an overabundance of vital force. But, just as he was articulating his germ theory, the language of Europe was being shot through with military metaphors. Politicians had also started using metaphors that cast the nation-state as a living being. Bad policy was a disease in the body politic.
So germs became an invading army. While the Prussians lay siege to Paris, Pasteur was saying that, in fermentation, germs laid siege to beer and wine. He pressed the analogy relentlessly. And when he wrote on public affairs, he said France had been enfeebled by revolution and rendered sterile by political theory.
For over a century, medicine has used those metaphors. AIDS stalks us; it uses many strategies in its attack. It invades and kills T-cells. Disease strikes the body's defenses. As doctors became soldiers at war with illness, the metaphor carried into medical practice.
Alternative medicine is less a body of technical knowledge than it is an attempt at linguistic reform. But, as it tries to claim legitimacy, it too slips back into military metaphors. It calls on the mind to marshal forces of good in the battleground of our body.
The only way we'll bring medicine into better alignment with our human nature, Montgomery says, is by heightening awareness. Just as we've had to do in areas of sexism and racism, we have to be aware of the words we use.
Medicine can be changed and, indeed, it must be. The military metaphor has run to the end of its usefulness. But we won't be able to make the needed changes until we've created a new language of medical discourse — until we've framed new metaphors.
Let's look at another linguistic and cultural shift in medicine: This one had gotten well underway by the time of Pasteur. As we'd entered the 17th century, physicians had forgotten most of the Hippocratic spirit of empiricism. The cure of disease turned less on observation than on exercises in logic. Like Hippocrates, physicians still believed treatment should address the whole body, but they'd let that idea wander strangely off track.
They believed disease was caused by gross imbalances of body fluxes and humors. They concentrated on treating these abstractions rather than what their eyes and other senses told them.
During the 1600s, that began changing in Italy, the new center of medical science and anatomy. Italian anatomists (of whom the Englishman Harvey was one, by the way — he studied there) were learning how the body worked, but not how to localize disease. They kept trying to cure the patient by adjusting body humors.
As the seventeenth century ended, a young man named Giovanni Morgagni entered medical school at Bologna. He graduated in 1701. From then on, he worked to make sense of disease, using anatomy and dissection.
Sixty years later he published a book titled: The Seats and Causes of Disease Investigated by Anatomy. In it, he set the foundations of pathological anatomy. The key word in his title was Seats. Morgagni showed that understanding disease meant seeing where it's seated within the body.
Doctor Reiser sums up Morgagni's new doctrine with a great phrase. Morgagni, he says, told us to look for the lesion within.
Four parts of Morgagni's book dealt with the head, the belly, the thorax, and generalized disease. But it was the fifth, a meticulous index, that was key to the other four.
By including that index, Morgagni kept sight of the whole body as he led us to seats of illness in its various parts.
He gave us far more than a museum of case histories. He offered a road map at the same time he took us on the trip. When Morgagni was done, clinicians and scientists alike had been offered means for tracing their way back to the common origins of symptoms.
Morgagni showed, beyond doubt, that specific disorders cause illness and death. Ruptured appendixes, syphilis of the aorta, epidural hematoma. A lifetime of compassion and clear thinking underlay this chamber of horrors. Modern medical thinking unfolds, case by case, as Morgagni gives us a new way to see illness.
His work was as radical and revolutionary as it was steady and methodical. Morgagni's religious and humanitarian convictions drove him to work without haste and without rest until he was 89. He was still going strong when he died of a stroke in 1771.
Morgagni told doctors to look for the lesion within. He called them to start identifying disease with abnormalities we can't see from outside. To do that, he'd found a new purpose for dissection. Doctors had dissected since Galen. But they'd only done it after the fact to see how the body worked.
The problem was, Morgagni couldn't yet change medicine because doctors still had no means for looking inside the bodies of living patients. And without means, they also had no concept.
So Stanley Reiser asks you to imagine yourself as a late-18th-century doctor with a patient who complains of, say, a pain in his side. Whatever's wrong, all you can do is count his pulse and feel his forehead. You can look for changes in skin tone. You can listen to his own report of symptoms. The only information you can conceive of collecting is external.
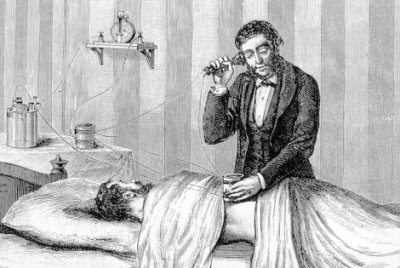
A big step away from that mindset occurred one day in 1816. A young French doctor, René Laënnec, was trying to diagnose a heart disorder in an obese young woman. He'd tried thumping her chest, but she was too heavy.
Even that was radical behavior for a doctor 200 years ago. Laënnec was engaging in more physical contact than was generally accepted. And, with his overweight patient, the sound told him nothing.
If Laënnec was radical, he wasn't radical enough to take the next logical step of putting an ear to the young lady's chest. That would've really crossed the line of acceptable behavior. So what was he to do!
Laënnec had an idea. He rolled a sheaf of papers into a tube. He placed one end on her chest and his ear on the other end. He was able to make out what was going on in her heart. He'd just created the first stethoscope. Three years later he published a book describing his design of a wooden stethoscope and its use.
By the 1830s, stethoscopes appeared with pliable rubber tubes, then binaural ones with earplugs. And, in counterpoint, debate raged over the changing tactics of diagnosis.
Understand Laënnec's dilemma with that patient: It wouldn't have been a dilemma for most doctors around him. In 1816, few doctors considered such diagnostics as thumping the thorax — much less putting an ear to the heart.
Diagnoses were based on looking at a patient and listening to the patient's own story. Doctors seldom questioned what patients said about themselves. Physical contact seldom went beyond counting a pulse or touching a forehead.
Of course Laënnec's ideas about thumping, feeling, and placing an ear to a patient went way back to Hippocrates. Hippocrates believed that all our senses should be used in diagnosis.
An ancient Greek doctor might've diagnosed diabetes by tasting a patient's urine. That kind of intimacy did not appeal to early-19th-century sensibilities!
Now stethoscopes let doctors keep their distance and still engage actual symptoms. You know perfectly well that stethoscopes don't really do better than an ear to the chest — but they do give you distance.
This simple new instrument became the signal to begin developing the techniques of a whole new kind of medicine — one in which doctors by-passed the patient's story and looked inside the patient's body for direct evidence of disease — for the lesion within.
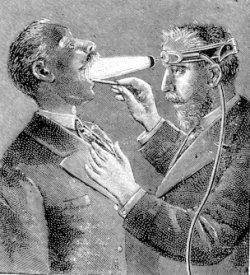
After stethoscopes came ophthalmoscopes, laryngoscopes, X-rays, CAT-scans, and MRI. The odd thing about all that is that it has, at last, intensified the old debate over how much doctor/patient intimacy is appropriate.
The stethoscope once promised to bridge the gap, to give some contact with patients' symptoms back to doctors. But it also gave doctors a way to stand even further away from patients.
Now the fun begins. For these new instruments of internal exploration all had about them an indisputable masculinity. They were almost all phallic in construction and use.
They entered the body. With them came a masculine vocabulary. The thrust of the 19th-century doctor was to engage in combat with disease. He waged war upon it. In an odd way, Morgagni and Laënnec had set us up to accept Pasteur's biomilitarism.
Lest you think I speak Freudian clap-trap here, I ask you to look at forceps: In the 18th century, babies were largely delivered by midwives. And midwives were, as they had always been, the agents of family planning. They instructed women in means of birth control and even helped them to terminate pregnancies.
But a new force was rising during those years. It was the force of mercantile economics. Mercantilism used two kinds of exploitation to balance trade. One was the use of colonies to supply raw materials.
The other kind of exploitation was creating a large lower class to manufacture goods for sale. That meant fostering childbirth among the poor.
So midwives collided with the mercantile agenda. Historian Lhonda Schiebinger tells how university-educated physicians — all males — took an interest in childbirth.
You see, midwives had no access to schooling. They were often illiterate. They trained by apprenticeship. Now the medical schools created a new professional called a man-midwife, and they armed him with surgical instruments, whose use was denied to women.
And so, armed with a forceps, means for entering the body, the man midwife began assisting birthing. Forceps could certainly be a blessing. But, like many of the drugs in our arsenal (interesting word) today, doctors overused them and damaged babies.
Midwives had worked around difficult births with gentle tricks of repositioning. Man-midwives were often reckless with their tools. Birth assistance changed from succor among women to a profitable enterprise.
By the mid-18th century, medical professionals had midwifery under attack. In 1760 a midwife wrote a book on birthing. In it, she angrily charged that men were trying to "forge the phantom of incapacity" in women's minds.
Still, stethoscopes and forceps gave doctors permission to redirect medical attention inside the patient. Down through the 1800s, doctors became increasingly aware of the various lesions within: cancers, ulcers, embolisms.
During the 19th century, doctors' offices sprouted all kinds of new instruments to help them look into patients throats, eyes and ears — trying to get at the elusive lesion within the body.
Then that great moment in 1895: Wilhelm Roentgen, working with cathode ray tubes, suddenly found he had a kind of ray that could "see" through flesh, but not through bone. He gave us the X-ray, and seldom has anything so taken the public's imagination.
This new marvel set the inventive muse in motion. Right away magazine cartoons celebrated the idea. A man uses an X-ray viewer to see through a lady's hat at the theater — that sort of thing. Soon we'd all have X-ray viewers, and great the mischief would be.
The very next year a company came out with lead panties to protect women from prying eyes. A would-be poet wrote,
Not worth your while
That false, sweet smile,
Which o'er your features plays:
Thy heart of steel
I can reveal
By my cathodic rays!
By the time I was a little boy, that'd turned into stories about Superman's X-ray eyes. Meanwhile, real X-rays were cheap and accessible.
I didn't have X-ray eyes, but I could X-ray my feet in new shoes at the department store. That didn't last long: we were just catching on to the terrible hazards of X-rays. But in 1896 futurists had seized at the possibilities of seeing through opacity. That year, the president of Stanford University suggested we might soon use X-rays to read thoughts. Was that satire or serious? We don't know.
Edison was deadly serious when he set out to focus enough X-rays on the human skull to watch the brain at work.
So scientists and science-fictionists alike seized this new marvel with the speed of gossip. Most important, Roentgen really had given doctors a new and seemingly non-invasive means for looking right at the elusive lesion within.
And so, joining with Pasteur's military metaphor, medicine has focused increasingly accurate rays, ultrasound, and fiber-optical devices on the precise lesion within our bodies. We pay a price for any new technology, and we've certainly paid a price for this close focus.
Doctors and lay people alike are beginning to see that we need better means for focusing on the whole human organism. We cannot keep reducing illness to detached points within the body.
Disease does not exist in simple isolation. But medicine will have to struggle to find its way back to the tough problem of curing the whole body — instead of just one piece of it.
Now back to the idea of narrative — my own narrative: The dilemma of modern medicine came home to me in a dramatic way on the evening of last February 15. I was attacked by a hit-and-run driver while I was walking my dogs. A driver came at me under full acceleration, onto the grass, and tried to kill me. The police guessed it was a gang initiation rite.
The impact broke up the fibulas in both legs, and it absolutely trashed my left tibia. So the surgeons ran a titanium tube down my tibia, spearing its rubble like shish kebab, and they screwed the tube in place.
Then, five days after the surgery, I suffered a stabbing pain in my chest and an inability to breathe. I'd suffered a pulmonary embolism. The trauma had kicked loose a blood clot.
Seven more days in the hospital on blood thinners and aggressive pulmonary therapy. Seven more days getting my blood oxygen level back to normal.
I was lucky to be in the hands of the crack Herman Hospital trauma team — Red Duke's operation. Surgeons, pulmonary specialists, hematologists, radiologists, all converged and compared notes in a delicate ballet.
They pinpointed the lesions within me. But with carefully choreographed teamwork they also reconstructed my body as a single organism.
Today, I'm in a fine state of repair just because doctors are finally creating strategies for seeing the whole body at the same time they focus upon the lesion within.
At the same time, it was clear that the hardest part of that process was sustaining the liaison among specialists. They did a good job of unifying their work while I was in the hospital. But it was forced cooperation.
Each medical professional was focused on one specialty. Cooperation was built into the structure of the trauma team but it didn't come naturally or easily. And, once I left the hospital, I also left that coordination of specialties.
Now it was up to me to be sure the fragments of my recovery were synchronized: That my blood thinners were managed, that my bones were knitting on schedule and my muscles were rebuilding, that I used pain medication intelligently, and that I dealt with the aspect of my recovery that medicine was quickest to ignore — the post-traumatic stress of having been nearly murdered.
Now an internist steered me through specialists. But a patient still has to travel from specialist to specialist — to people who only talk with one another through the patient. And, it's woe betide a patient who trusts the coordination of his treatment to a traveling chart. That's asking for trouble. My narrative was the only binding tissue in the managed care process.
Medicine has learned to find the lesion within — the specific locus of trouble. But now medicine must master the terribly important task of putting those pieces together.
I am poignantly aware, after my own recent experience, just how very good you all are at pinpointing the seats of illness within. And you are very good.
But 21st century medicine faces a great gaping problem. How can medicine continue to be as adept as it is at locating the seat of disease or trauma — and now find means for addressing the whole affected organism?
The harmony of body and mind, is an essential part of healing the wound. Fail to find that unity, and the wound to the body will remain unhealed long after the skin has closed.
In the near wake of my assault, people constantly stopped to ask, "How are you doing?" After a while I realized that I wasn't helping anyone by playing the game, so I tried something. I answered one colleague by saying, "My leg hurts like Hell, and I'm so frigging tired of crutches I could sit down and cry." So what do you think happened:
He said, "Oh yes, well — but you are getting better, aren't you!" Friends needed my reassurance. What'd happened to me frightened them. They needed for me to allay their fear. And of course I'd done the same thing a thousand times when friends of mine were hurt
Now my story now elicited their stories. When I listened carefully I suddenly heard, for the first time, the pain that friends had been suffering in silence around me.
For years I'd been next to useless to friends with cancers, and other mind and body altering ills. Now they opened up to me. The exchange of stories granted me intimacy with friends that I'd never had before. So I underwent massive change. I saw my own mortality; I saw the goodness of people around me.
Meanwhile, my forever-flawed leg still hurts just enough to be a constant reminder of my new ethnicity.
Today's 19th century medical metaphors make it so hard for medicine to deal with these issues. Masculine medicine, 19th and 20th century medicine, equates doctors with warriors — hurling their spears and arrows at disease. You wrap the patient on the operating table in surgical linens that hide the face from view. War is objective business — conducted in a detached way. You don't look at the enemy's face or consider his story.
The regimen of authority and obedience is forged in medical school just the way it was forged when I was in army boot camp. Both institutions use the tool of sleep deprivation to mold recruits to the chain of command. Both are profoundly male worlds.
The result is that medicine is equipped to do a big part of the healing process — chiefly that part which does not require the stereotypical female virtues of succor and compassion. Medicine is at its best when it can treat the body without reference to the mind.
But, in the end, the body will not be healed independently of the mind. Not even so elementary thing as a broken leg. Today, I thank those skillful surgeons and pulmonary therapists who worked on me.
But I also thank myself — for putting optimism and determination into the healing process. If my mind had been in a slightly worse place, what happened to me could've brought me down.
If I'd believed that my doctors' healing powers were the whole story, I would've been over-drugged, beaten by pain and disability, fearful of using my damaged leg, and (worst of all) out of contact with the psychic wound I'd been dealt.
If I hadn't recognized the missing elements in modern medicine, and found my own means for patching them in, my wound would have been far greater than it was. If I hadn't sought out people who could actually hear my own narrative, I would've strangled on the horror of what'd happened to me.
I am forever grateful to the medical professionals who began my healing process, but I lament their inability to work beyond the first steps in that process.
You students will've achieved nothing if you simply join this existing world of 20th century medicine. You are obliged to change it as well. That change will take place. But what is true of any revolution will be true here:
The only people who survive revolutionary change are the ones who help to bring it about.
SOME ADDITIONAL SOURCES
Montgomery, S. C., The Scientific Voice. New York: The Guilford Press, 1996. (See especially, Chapter 3.)
Reiser, S. J., Medicine and the Reign of Technology, Cambridge: Cambridge University Press, 1978.
Knight, N., "'The New Light': X-rays and Medical Futurism," Imagining Tomorrow: History, Technology, and the American Future, (Joseph Corn, ed.) Cambridge, Mass.: MIT Press, 1986, Chapter 1.